Breathing and Exchange of Gases
|
|
Breathing: is a process of exchange of O2 from atmosphere and with CO2 produced by cells.
Mechanism of breathing differs from one group of animals to the other depending upon their habit. Lower invertebrates like sponges and flatworms exchange gases through body surface. Aquatic arthropods and molluscs use gills for breathing. Terrestrial animals use lungs for breathing and mammals have well developed respiratory system. |
Respiration in Human:
The atmospheric air that we breathe passes through nasal chamber, pharynx (common pathway for food and air), trachea, bronchi (primary, secondary and tertiary), bronchioles (initial and terminal) and alveoli.
Respiration involves:
- The wall of trachea, bronchi and initial bronchioles are supported by incomplete cartilaginous rings.
- The bronchi, bronchioles and alveoli comprise the lungs and each lung is covered by a double layer membrane called pleural membrane enclosing pleural fluid.
- Lung lies in the thoracic chamber, which is made up of sternum (ventral side), vertebral column (dorsal side), ribs (lateral side) and diaphragm (the base).
Respiration involves:
- Breathing, also called Pulmonary respiration.
- Diffusion of gases (CO2 and O2) at alveolar membrane.
- Transportation of gases by the blood.
- Exchange of gases between blood and tissue.
- Utilization of O2 by cells and release of CO2.
|
|
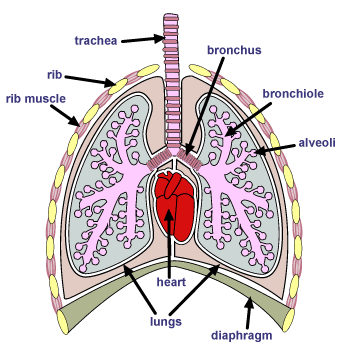
Diagram of human respiratory system.
|
Mechanism of Breathing:
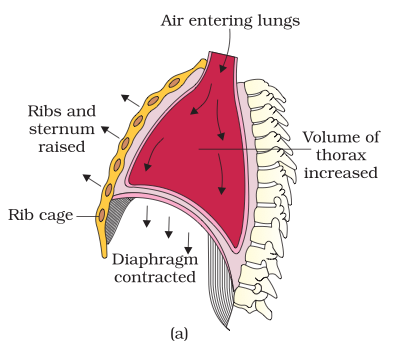
Breathing involves two steps: inspiration and expiration.
Inspiration: Contraction of diaphragm and external inter-costal muscles increase the thoracic volume leading to increase in pulmonary volume. Increase in pulmonary volume leads to decrease in intra-pulmonary pressure below the atmospheric pressure resulting in inflow of atmospheric air into the lungs. Diagrammatic representation of inspiration is shown (figure a) below.
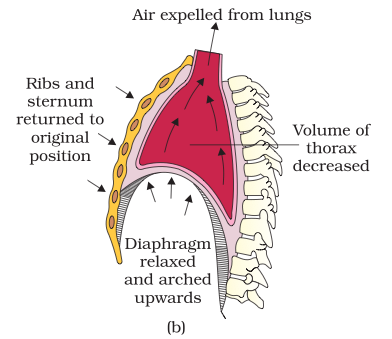
Expiration: Relaxation of diaphragm and contraction of inter inter-costal muscles leads to decrease in thoracic volume leading to decrease in pulmonary volume. Decrease in pulmonary volume leads to increase in intra-pulmonary pressure above the atmospheric pressure resulting in outflow of pulmonary air into the atmospheric air. Diagrammatic representation of expiration is shown (figure b) below.
Inspiration: Contraction of diaphragm and external inter-costal muscles increase the thoracic volume leading to increase in pulmonary volume. Increase in pulmonary volume leads to decrease in intra-pulmonary pressure below the atmospheric pressure resulting in inflow of atmospheric air into the lungs. Diagrammatic representation of inspiration is shown (figure a) below.
Expiration: Relaxation of diaphragm and contraction of inter inter-costal muscles leads to decrease in thoracic volume leading to decrease in pulmonary volume. Decrease in pulmonary volume leads to increase in intra-pulmonary pressure above the atmospheric pressure resulting in outflow of pulmonary air into the atmospheric air. Diagrammatic representation of expiration is shown (figure b) below.
Inspiration
|
Expiration
|
Respiratory Volumes and Capacities:
Tidal Volume (TV):
Volume of air inspired or expired during a normal respiration. It is approx. 500 mL., i.e., a healthy man can inspire or expire approximately 6000 to 8000 mL of air per minute.
Inspiratory Reserve Volume (IRV):
Additional volume of air, a person can inspire by a forcible inspiration. This averages 2500 mL to 3000 mL.
Expiratory Reserve Volume (ERV):
Additional volume of air, a person can expire by a forcible expiration. This averages 1000 mL to 1100 mL.
Residual Volume (RV):
Volume of air remaining in the lungs even after a forcible expiration. This averages 1100 mL to 1200 mL.
By adding up a few respiratory volumes described above, one can derive various pulmonary capacities, which can be used in clinical diagnosis.
Inspiratory Capacity (IC):
Total volume of air a person can inspire after a normal expiration. This includes tidal volume and inspiratory reserve volume (TV+IRV).
Expiratory Capacity (EC):
Total volume of air a person can expire after a normal inspiration. This includes tidal volume and expiratory reserve volume (TV+ERV).
Functional Residual Capacity (FRC):
Volume of air that will remain in the lungs after a normal expiration. This includes ERV+RV.
Vital Capacity (VC): The maximum volume of air a person can breathe in after a forced expiration. This includes ERV, TV and IRV or the maximum volume of air a person can breathe out after a forced inspiration.
Total Lung Capacity: Total volume of air accommodated in the lungs at the end of a forced inspiration. This includes RV, ERV, TV and IRV or vital capacity + residual volume.
Volume of air inspired or expired during a normal respiration. It is approx. 500 mL., i.e., a healthy man can inspire or expire approximately 6000 to 8000 mL of air per minute.
Inspiratory Reserve Volume (IRV):
Additional volume of air, a person can inspire by a forcible inspiration. This averages 2500 mL to 3000 mL.
Expiratory Reserve Volume (ERV):
Additional volume of air, a person can expire by a forcible expiration. This averages 1000 mL to 1100 mL.
Residual Volume (RV):
Volume of air remaining in the lungs even after a forcible expiration. This averages 1100 mL to 1200 mL.
By adding up a few respiratory volumes described above, one can derive various pulmonary capacities, which can be used in clinical diagnosis.
Inspiratory Capacity (IC):
Total volume of air a person can inspire after a normal expiration. This includes tidal volume and inspiratory reserve volume (TV+IRV).
Expiratory Capacity (EC):
Total volume of air a person can expire after a normal inspiration. This includes tidal volume and expiratory reserve volume (TV+ERV).
Functional Residual Capacity (FRC):
Volume of air that will remain in the lungs after a normal expiration. This includes ERV+RV.
Vital Capacity (VC): The maximum volume of air a person can breathe in after a forced expiration. This includes ERV, TV and IRV or the maximum volume of air a person can breathe out after a forced inspiration.
Total Lung Capacity: Total volume of air accommodated in the lungs at the end of a forced inspiration. This includes RV, ERV, TV and IRV or vital capacity + residual volume.
Exchange of Gases:
|
|
Solubility: solubility of CO2 is 20-25 times greater than the solubility of O2, therefore, greater amount of CO2 will diffuse across a diffusion membrane than O2. |
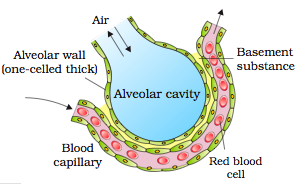
Diagram of a section of an alveolus.
Source: cbse
|

Table of partial pressure of O2 and CO2 at different part. Source: cbse.
|
Transport of Gases (O2 and CO2):
Transport of Oxygen (O2):
- ~ 97% of O2 transported by RBC.
- ~ 3% of O2 transported by plasma in dissolved form.
- Oxygen will bind with hemoglobin in reversible manner to form oxyhemoglobin.
- Binding of oxygen to hemoglobin is primarily related to partial pressure of O2.
- Hemoglobin can carry a maximum of four O2 molecule.
- At alveoli where there is high PO2, low PCO2, H+ concentration, and temperature, oxygen will bind with hemoglobin to form oxyhemoglobin. At tissue site where there is low PO2, high PCO2, H+ concentration and temperature, dissociation of O2 from oxyhemoglobin will take place.
- Every 100 ml of oxygenated blood can deliver around 5 ml of O2 to tissues.
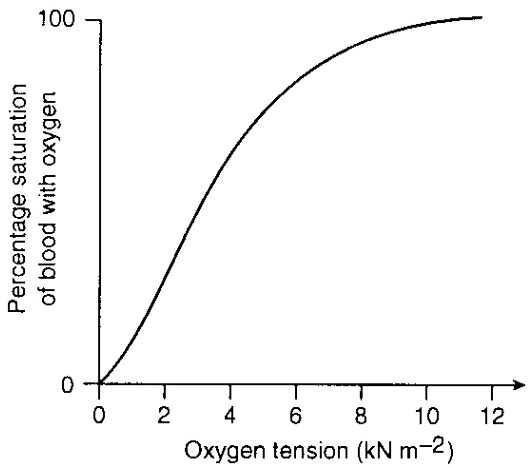
Oxygen dissociation curve
Transport of Carbon Dioxide (CO2):
In tissue where there is high PCO2, H+ concentration and temperature and low PO2, oxygen will bind with haemoglobin to form carbamino-haemoglobin. At alveoli where there is high PO2 and low PCO2, H+ concentration and temperature, dissociation of CO2 from carbamino-haemoglobin will take place.
- ~ 25% of CO2 transported by RBC.
- ~ 5% of CO2 transported by plasma in dissolved form.
- ~ 70% of CO2 transported as bicarbonates.
- Every 100 ml of deoxygenated blood can deliver 4 ml of CO2 to alveoli.
- RBC contain high concentration of enzyme ( Carbonic anhydrase ) which facilitate the following reaction:

At tissue site, CO2 diffuses into the plasma and the reaction proceeds in forward direction whereas at alveoli, the reaction proceeds in reverse direction and the CO2 diffuses into the alveoli.
Regulation of Respiration:
- Respiration is moderated by nervous system.
- Respiratory rhythm centre (medulla region) and pneumotaxic centre (Pons region) are responsible for regulation of respiratory rhythm.
- A chemosensitive area near rhythm centre and receptor associated with aortic arch and carotid artery can recognize change in CO2 and H+ concentration and send message to the rhythm centre for remedial actions.
Respiratory Disorders:
Asthma: difficulty in breathing due to inflammation of bronchi and bronchioles.
Emphysema: disorder in which respiratory surface is reduced due to damaged alveoli.
Emphysema: disorder in which respiratory surface is reduced due to damaged alveoli.
HTML Comment Box is loading comments...
|
|
